Novica Kos-Amyotrophic Lateral Sclerosis (ALS)-(Serbian)
 Patient's Name: Novica Kos
Patient's Name: Novica Kos
Gender: Male
Age: 50 years old
Nationality: Serbian
Diagnosis: Amyotrophic Lateral Sclerosis (ALS)
Condition Upon Admission:
The patient was admitted to the hospital with a diagnosis of Amyotrophic Lateral Sclerosis mainly due to "progressive limb weakness accompanied by dysarthria for more than 8 months". His main symptoms included progressive weakness of all limbs, difficulty in grasping with both hands, and frequent joint pain. He had trouble walking, along with pain in the left knee joint. His speech was slurred and slow, while his mental status was fair. He had previously taken riluzole for treatment but discontinued the medication due to severe side effects.
Physical Examination on Admission:
The patient’s heart rate was 70 beats per minute, respiratory rate 20 breaths per minute, blood pressure 128/79 mmHg, and blood oxygen saturation 96%. He had a normal build and body habitus. No obvious cyanosis was observed on the lips. Breath sounds of both lungs were unremarkable. Heart sounds were strong with a regular rhythm, and no significant murmurs were heard over each valvular area of the heart. The abdomen was flat and soft; neither the liver nor the spleen was palpable below the costal margins. No obvious edema was noted in both lower extremities.
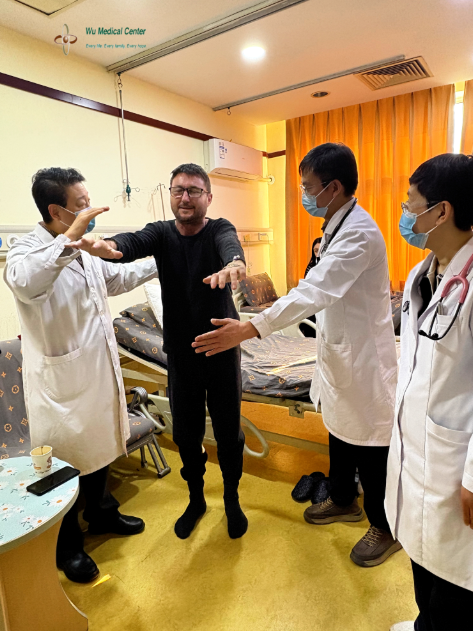
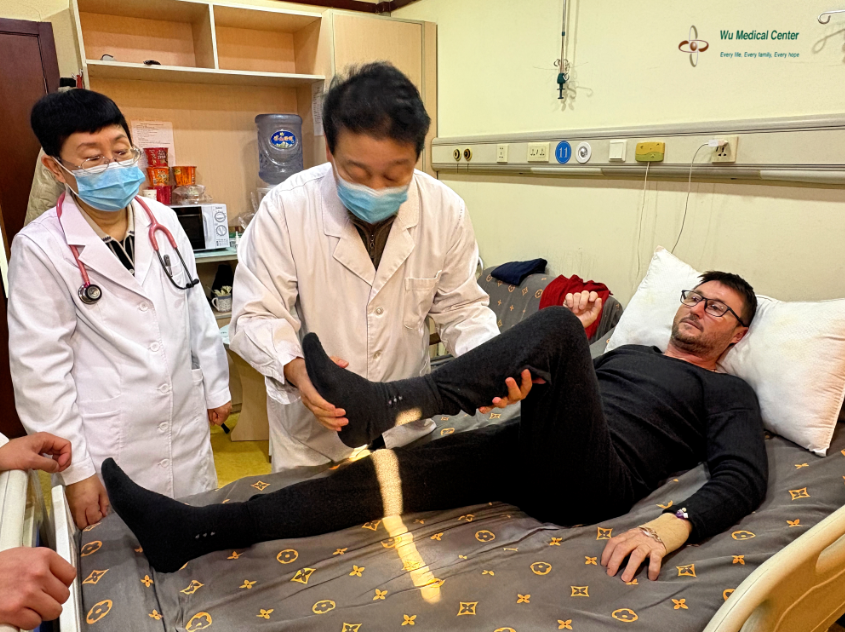
Neurological Examination:
The patient was conscious with a fair mental status. His speech was slurred and slow, presenting with a sighing quality. His memory and calculation abilities were normal. Eye movements were flexible in all directions. Mild atrophy of the lingual muscles was noted, with decreased flexibility of tongue movement. His masticatory and swallowing functions were slightly impaired: he could consume solid foods but occasionally experienced choking fits when ingesting liquids. The elevation strength of bilateral soft palates was diminished. The neck was supple; muscle strength for neck rotation and shoulder shrugging was Grade 3, with poor resistance to external force. Limb muscle strength was reduced, with the left side more significantly affected: muscle strength of the left upper limb was Grade 3, right upper limb Grade 3+; left hand grip strength was Grade 2, right hand grip strength Grade 3+. He was barely able to grasp with his left hand, and finger strength was poor bilaterally—he could hold a pen only with his left thumb and index finger (the remaining three fingers were non-functional); his right hand could hold a pen but could not resist external force. Atrophy of the thenar, hypothenar, and interosseous muscles was observed in both hands. Mild fasciculations were present in the limbs. Muscle strength of the left lower limb was Grade 3, right lower limb Grade 4, and he was unable to stand on a single foot. He required bimanual support to rise from a bed or sofa, with a slow movement speed. Limb muscle tone was increased, and tendon reflexes were hyperactive. Pathological reflexes were positive in all limbs. Superficial and deep sensations were normal. Rapid alternating hand movements were slow, and the finger-opposition test had poor completion (only the index fingers of both hands could complete the movement bilaterally). The finger-to-nose test could be completed slowly with both hands, while the heel-knee-tibia test was completed slowly and clumsily on both sides. Meningeal irritation signs were negative.
Treatment Process:
The patient was clearly diagnosed with Amyotrophic Lateral Sclerosis upon admission. During hospitalization, he was administered neural stem cell therapy to repair motor nerve damage, along with mesenchymal stem cell therapy to provide neurotrophic, endocrine, and immune support. Adjuvant CAST therapy was given with medications including edaravone, riluzole, neurotrophic factors, and reduced glutathione. Comprehensive rehabilitation therapy was also implemented in combination with the above treatments.
Post-Treatment Condition:
The patient’s speech becomes clearer than before. His limb strength is improved significantly: the muscle strength of both upper arms and forearms is reached Grade 5-, and he can resist considerable external force when shrugging his shoulders and flexing/extending the biceps and triceps. The grip strength of his left hand is Grade 4+, and that of his right hand is Grade 5-; he can grasp others’ fingers with both hands, with a marked improvement in resistance ability. The strength of his fingers is increased: he can hold a pen with all fingers of his left hand and resist external force; his right hand can hold a heavier penlight and also resist external force. His finger-opposition test performance is more flexible than before—he can now complete the movement with both the middle and ring fingers bilaterally. The speed of his rapid alternating hand movements is increased and becomes more agile. The muscle strength of both lower limbs is basically Grade 5, and he performs much better on the bilateral heel-knee-tibia test than previously. His limb muscle tone returns to basically normal. Joint pain is significantly relieved. Tendon reflexes of both upper limbs are normal, while those of both lower limbs are slightly increased. He can stand on each leg unilaterally for up to 10 seconds at maximum. He is able to stand up from a seated position and a low position independently without arm support, with a notable improvement in speed and flexibility during the movement.